NEMT Claim Denials: Causes, Codes & How to Reduce Them in 2026
NEMT claim denials quietly eat into provider revenue every month. Here's what causes them, how to read the denial codes, and how to bring your denial rate down in 2026.
Quick answer
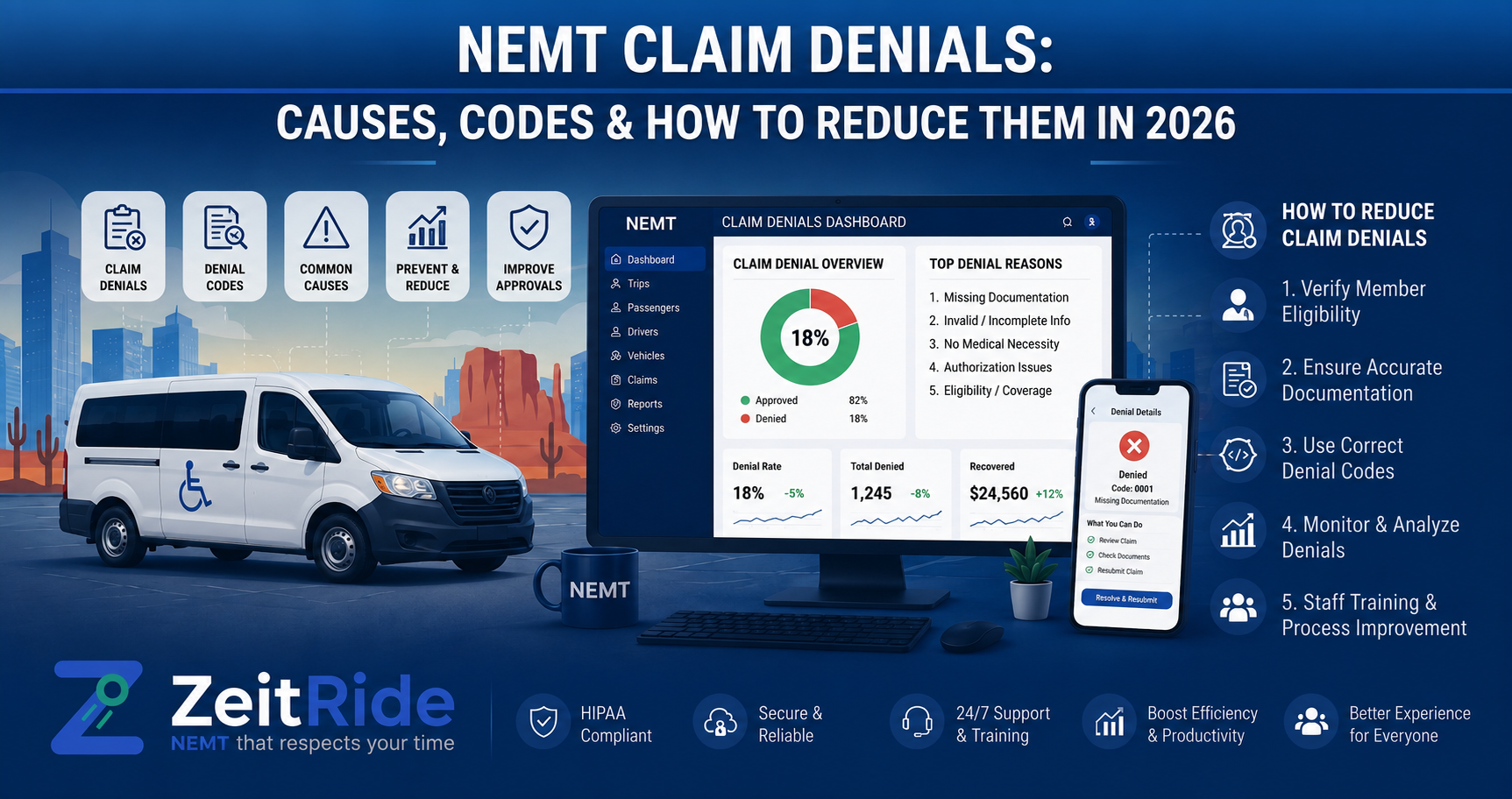
NEMT claim denials mostly stem from missing prior authorization, incomplete trip documentation, incorrect HCPCS coding, and Medicaid eligibility mismatches. Providers reduce denials by verifying eligibility before every trip, capturing GPS and proof-of-delivery data automatically, and scrubbing claims before submission.
ZeitRide Team
NEMT Operations Expert
A denied claim isn't just a paperwork problem — it's a trip you already paid a driver for that you're not getting reimbursed for. NEMT claim denials are one of the most persistent revenue leaks in this industry, and most of them share the same handful of root causes: missing authorization, incomplete documentation, and coding errors. This guide breaks down why denials happen, what the denial codes actually mean, and a practical framework for bringing your denial rate down.
NEMT Claim Denials vs. Rejections: What's the Difference?
These two terms get used interchangeably, but they're not the same thing, and mixing them up wastes time you don't have. A rejection happens before a payer ever reviews your claim — it's kicked back for a technical error like a missing field or an invalid ID, and you simply correct it and resubmit. A denial happens after the payer has reviewed and processed the claim, and it means they've decided not to pay, usually for a substantive reason like missing prior authorization or insufficient documentation. Denials require an appeal, not just a resubmission — which is why they take longer and cost more to resolve.
- Rejection: Happens before adjudication, caused by technical/formatting errors, fixed by correcting and resubmitting
- Denial: Happens after adjudication, caused by substantive issues (authorization, documentation, eligibility), resolved through formal appeal
- Why it matters: Treating a denial like a rejection — just resubmitting without addressing the underlying issue — usually results in a second denial
Reasons for NEMT Claim Denials
Most NEMT claim denials come from a small set of recurring problems, and the pattern is remarkably consistent across states and brokers. Understanding which category your denials fall into is the first step toward actually fixing the underlying process instead of just resubmitting and hoping.
Missing or Expired Prior Authorization
Many NEMT trips require pre-authorization before the ride happens, and this is one of the most common denial triggers in the industry. If the authorization was never obtained, expired between scheduling and the trip date, or doesn't match the service level billed, the claim gets denied — even if the transport itself was medically necessary and completed without issue.
Incomplete or Inconsistent Documentation
This is the single largest denial category. A trip manifest with mismatched pickup and drop-off times, a missing signature, or no evidence tying the transport to a covered medical appointment will trigger a denial. Our NEMT EVV compliance guide covers exactly what documentation states now require to close this gap.
Eligibility Mismatches
Medicaid eligibility isn't static — it can change mid-month. A trip scheduled weeks in advance for a patient who was eligible at booking but not on the actual service date results in an automatic denial, regardless of how well the trip itself was executed.
Incorrect HCPCS Codes or Modifiers
NEMT billing depends on precise HCPCS codes and origin/destination modifiers. Billing a wheelchair transport code when the patient was ambulatory, or using an outdated modifier, triggers an immediate denial even when every other part of the claim is accurate.
Duplicate or Late Submissions
Submitting the same claim twice, or missing a payer's filing deadline (often 90 days or less, and shorter for some state Medicaid programs), results in denial regardless of the claim's underlying validity.
Common NEMT Denial Codes Explained
When a claim is denied, the payer communicates why through standardized codes on your Explanation of Benefits (EOB) or Electronic Remittance Advice (ERA). CARC (Claim Adjustment Reason Codes) explain the category of the problem; RARC (Remittance Advice Remark Codes) point to the specific missing field or required fix. Read them together — the CARC tells you what went wrong, the RARC tells you how to fix it.
| Denial Code | Meaning, Cause & Resolution | ||
|---|---|---|---|
| Code | Meaning | Typical Cause | How to Resolve |
| CO-16 | Claim lacks information needed for adjudication | Missing field or documentation | Check RARC for the specific missing element, correct, and resubmit |
| CO-197 | Precertification/authorization absent | No prior authorization on file | Submit retro-auth request if allowed by payer; appeal with trip documentation |
| CO-29 | Time limit for filing has expired | Claim submitted after payer's filing deadline | Appeal with proof of timely filing if applicable, otherwise generally non-recoverable |
| CO-18 | Duplicate claim | Same claim submitted more than once | Verify submission history before resubmitting; do not resend without checking |
| CO-50 | Non-covered service — not deemed medically necessary | Missing or insufficient medical necessity documentation | Submit Physician Certification Statement (PCS) and trip records |
| PR-204 | Service not covered under patient's plan | Eligibility or plan-coverage mismatch | Verify eligibility on the actual date of service, not the scheduling date |
How Broker-Specific Denial Patterns Differ
If you work with multiple brokers — ModivCare, MTM, Veyo, or a state Medicaid system directly — you'll notice each has its own denial tendencies. Some brokers deny heavily on GPS-to-billed-mileage mismatches, others focus more on wheelchair-versus-ambulatory coding accuracy. Tracking denial codes by broker, not just in aggregate, usually reveals which relationship needs the most process attention.
How to Appeal a Denied NEMT Claim
Nearly every denied NEMT claim can be disputed, and a well-documented appeal has a meaningfully better chance of success than a resubmission without changes.
- Identify the exact denial reason from the CARC/RARC codes on your EOB or ERA
- Gather supporting documentation — trip manifests, GPS logs, signatures, and PCS if applicable
- Submit the appeal through the correct channel (broker portal for ModivCare/MTM/Veyo, or the state Medicaid system directly)
- Track the payer's specific appeal window — typically 30 to 120 days depending on the payer
- Follow up in writing and keep a record of every submission and response
How to Reduce NEMT Claim Denials
Prevention is far cheaper than appeals. Most operators who bring their denial rate down do it by tightening the same four points in their workflow.
- Verify eligibility before every trip, not just at scheduling — eligibility can change between booking and service date
- Capture GPS and proof-of-delivery data automatically during the trip, rather than relying on manual driver logs
- Scrub claims before submission to catch coding and authorization gaps before the payer ever sees them
- Track denials by code and by broker so you can fix the root cause instead of the individual claim
- Train staff quarterly on current HCPCS codes and modifier rules, since these change periodically by state
When evaluating whether your current tools support this, our guide on how to choose NEMT software walks through exactly which capabilities matter for denial prevention specifically.
What's a Normal NEMT Denial Rate?
Denial rates vary by operator size and billing maturity, but industry-reported estimates commonly place first-submission NEMT denial rates in the range of 10–20%, with smaller or newer operators sometimes seeing higher figures. If your rate is meaningfully above that range, it's usually a sign of a specific, fixable process gap rather than something to accept as a cost of doing business — most denials in this range are documentation or authorization issues, both of which are preventable with the right workflow.
How the Right Billing Workflow Prevents Denials
Most denial-prevention advice comes down to one thing: closing the gap between what happens on the trip and what gets submitted on the claim. When GPS timestamps, electronic signatures, and trip data flow automatically from dispatch into billing — instead of being re-entered by hand — the documentation and coding errors that cause the majority of denials simply don't happen. Our best billing software for NEMT providers breakdown compares what to look for if your current process still relies on manual data entry between systems.
Frequently Asked Questions
Q: What's the difference between an NEMT claim denial and a rejection?
A rejection happens before the payer reviews the claim, usually due to a technical error, and is fixed by correcting and resubmitting. A denial happens after the payer reviews and processes the claim, and requires a formal appeal with supporting documentation to resolve.
Q: What's the most common cause of NEMT claim denials?
Missing or incomplete documentation — particularly trip manifests, signatures, and prior authorization — is consistently reported as the leading cause of NEMT claim denials.
Q: How long do I have to appeal a denied NEMT claim?
Appeal windows vary by payer, typically ranging from 30 to 120 days from the denial date. Always confirm the specific timeline with the broker or state Medicaid portal that issued the denial.
Q: Can NEMT software actually reduce my denial rate?
Yes — software that automatically captures GPS, timestamps, and electronic signatures during a trip and feeds that data directly into billing eliminates many of the documentation and re-entry errors that cause denials in the first place.
Q: What is a normal NEMT claim denial rate?
Industry-reported estimates commonly place first-submission denial rates around 10–20%. Rates meaningfully above that typically point to a specific, fixable gap in documentation or authorization workflows.
Every denied claim is a trip you already paid for. If your denial rate feels higher than it should be, it's worth seeing exactly where the documentation gap is happening — talk to the ZeitRide team about how automated dispatch-to-billing workflows close that gap before claims are ever submitted.
Rather see it than read about it?
Bring a real route, a couple of drivers, and your current process. 15 minutes, zero pitch.